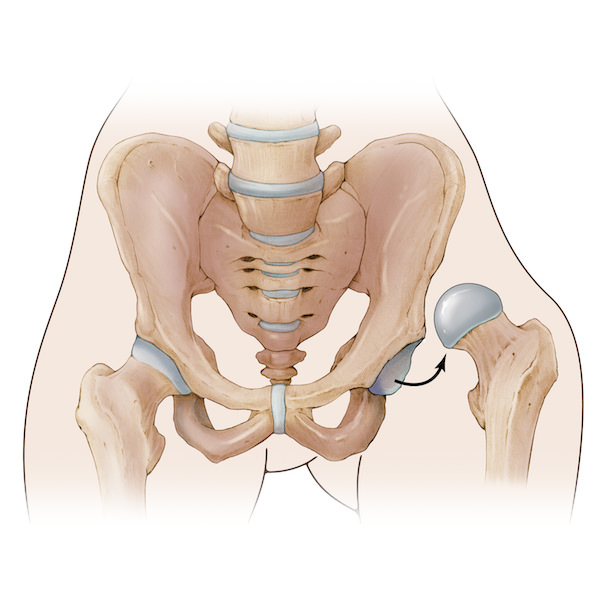
The surgical hip dislocation approach is a combination of the posterior-lateral approach with a trochanteric flip and anterior dislocation of the hip. The advantage of this technique is access to the entire hip joint without compromising the blood supply to the femoral head.


Overview

Indications / Candidacy
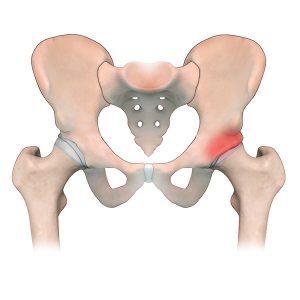
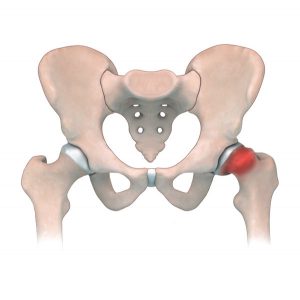
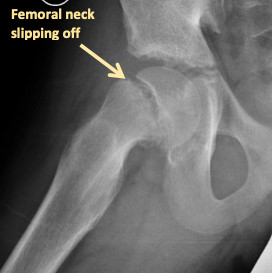
Surgical hip dislocation can be used to correct a slipped deformity of the femoral head, or impingement of the femoral neck or acetabulum that can be found in both SCFE and Femoral-acetabular impingement. Both of these conditions can cause pain and damage to the hip joint that affects a patient’s ability to comfortably perform activities.
Good candidates for this surgery may have:
- Previous trauma to the hip leading to deformities of the head and neck of the femur
- SCFE (slipped capital femoral epiphysis)
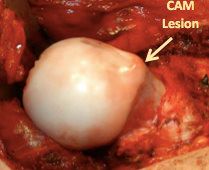
- Femoral-acetabular impingement (FAI) and labral tears
- Pain related to poor hip biomechanics that worsens with activity
- Painful and decreased range of motion related to hip deformities
Treated Conditions
The Canadian Limb Lengthening Center offers a team of experienced surgeons, nurses and physiotherapists that make patients feel supported throughout their entire treatment process. Our ability to treat complex orthopedic conditions with a holistic approach gives our patients the best possible outcomes. We pride ourselves in providing highly specialized, expert care that helps patients and families dealing with Perthes disease, among many other diseases. To learn more about conditions treated using surgical hip dislocation, follow the links below:

Surgical Technique
SCFE
- The patient is placed on the table in a lateral position (on the side).
- A lateral skin incision is made.
- The leg is internally rotated so we can see the posterior border of the gluteus medius muscle. This muscle is traced to the posterior ridge of the vastus lateralis muscle.
- A 1.5cm thick trochanteric osteotomy is performed following the trace mentioned above using a saw.
- The soft tissues are pulled aside and an incision is made of the anterolateral surface of the hip capsule.
- The hip is then dislocated anteriorly by flexing and externally rotating the femur.
- The leg is then placed in a sterile bag over the front of the table
- The surgeon can now access the femoral head and the acetabulum and address the pathology as needed.
- A 2.0mm hole is drilled in the femoral head to document preservation of the blood supply and assess viability of the head during this portion of the surgery.
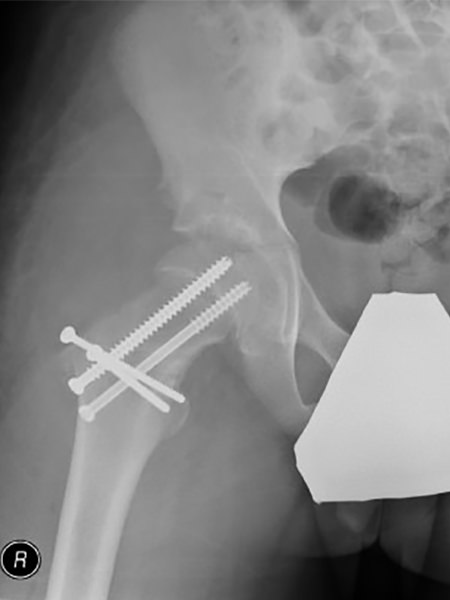
- If unstable, prior to dislocating the hip, 2 K-wires are placed to secure the head to the neck.
- Once dislocated, the neck periosteum (layer of fascia around the bone) of the femur is cut and peeled (like a banana) on the anterior-lateral portion of the neck to preserve the blood supply to the femoral head.
- The neck is exposed to be able to reposition the head on the neck and two large screws are used to fix it in place.
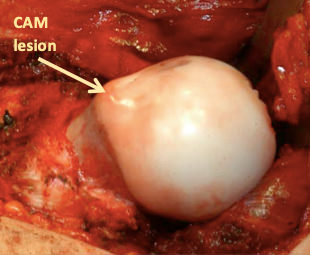


FAI
- The patient is placed on the table in a lateral position (on the side).
- A lateral skin incision is made.
- The leg is internally rotated so we can see the posterior border of the gluteus medius muscle. This muscle is traced to the posterior ridge of the vastus lateralis muscle.
- A 1.5cm thick trochanteric osteotomy is performed following the trace mentioned above using a saw.
- The soft tissues are pulled aside and an incision is made of the anterolateral surface of the hip capsule.
- The hip is then dislocated anteriorly by flexing and externally rotating the femur.
- The leg is then placed in a sterile bag over the front of the table
- The surgeon can now access the femoral head and the acetabulum and address the pathology as needed.
- A 2.0mm hole is drilled in the femoral head to document preservation of the blood supply and assess viability of the head during this portion of the surgery.
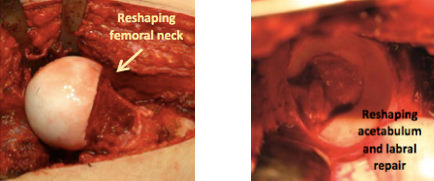
- For pincer impingement, the labrum is detached from the acetabulum like a bucket handle and the overhanging bone of the acetabulum is removed.
- The labrum is then re-attached using anchors
- The femoral neck is then assessed for CAM lesions and reshaped to ensure that there is no impingement
- The hip is then reduced by applying manual traction on the flexed knee followed by internal rotation and extension.
- The wound is irrigated and the capsulotomy is closed with a vicryl suture.
- The greater trochanter is secured using two 3.5mm cortical screws directed towards the lesser trochanter.
- The tensor fascia lata and soft tissues, as well as the skin, are then closed.
Results
Surgical hip dislocation improves lower limb length discrepancy, gait, and range of motion at the hip for patients. The result from surgery can improve hip biomechanics and function. Our patients see improvements in quality of life after surgery and experience less complications, pain and discomfort later in life. This approach allows for repair of intra-articular structures and may help prevent osteoarthritis from progressing in future.


Potential Complications
As with any surgical procedure, the Surgical hip dislocation technique can have difficulties and complications. In most cases, our team of specialist can address these concerns without compromising the end results or outcome. Complications and side effects may include:
- Avascular necrosis (AVN) of the femoral head
- Nerve injury to the sciatic nerve (Neuropraxia)
- Trochanteric non-union or malunion
- Heterotopic ossification
- Infection of the bone (osteomyelitis)
- Progression of arthritis
- Neurovascular injury (rare)
- Deep vein thrombosis (rare)
Case studies
AM I A CANDIDATE?
Are you experiencing an orthopedic condition and would like to improve your physical capabilities?
Or you simply would like to achieve your long-lasting dream of improving your height?
Let us help you achieve your optimal health and wellness in a professional setting.
Let’s open up a discussion to help you achieve your goals.
Highly specialized expert care at CLLC
At the Canadian Limb Lengthening Centre we offer complex deformity correction and limb lengthening surgeries performed by experienced surgeons with the most up to date technologies. When it comes to your care, and treatment of deformity and limb length discrepancy, our surgeons have extensive training and experience.
