Both congenital femoral deficiency (CFD) and Fibular hemimelia can be addressed using reconstructive surgeries of the hip, knee, and ankle. These procedures can be referred to as SUPER Knee, SUPER Hip and SUPER Ankle surgeries. SUPER is an acronym for Systematic Utilitarian Procedure for Extremity Reconstruction. These surgeries work to reconstruct soft tissue, realign bone, and correct contractures prior to proceeding with limb lengthening surgeries. In most cases it is preferred that patients be between the ages of 2-4, however surgery can be performed as late as adulthood as well.


Overview

Indications / Candidacy
Congenital femoral deficiency (CFD) presents a spectrum of deficiency, deformity and dysplasia of the upper femur, hip joint and acetabulum. Fibular hemimelia is a rare condition in which part of the fibula (bone in the lower leg) is missing. Both of these deformities can result in lack of integrity, instability and limited mobility of the hip, knee and ankle joints.
Good candidates for reconstructive surgeries may experience:
- Hip/knee dysplasia
- Bone deformities and malrotation
- Soft tissue contractures of the hip and knee
- A deformity that is present at birth
- Knee, hip or ankle deformity
- Limb length discrepancies
Treated Conditions
The Canadian Limb Lengthening Center offers a team of experienced surgeons, nurses and physiotherapists that make patients and their families feel supported throughout their entire treatment process. Our ability to treat complex congenital limb deformities with a holistic approach gives our patients the best possible outcomes. We pride ourselves in providing highly specialized, expert care. To learn more about Congenital femoral deficiency (CFD) and Fibular hemimelia (FH), follow the link below:

Surgical Technique
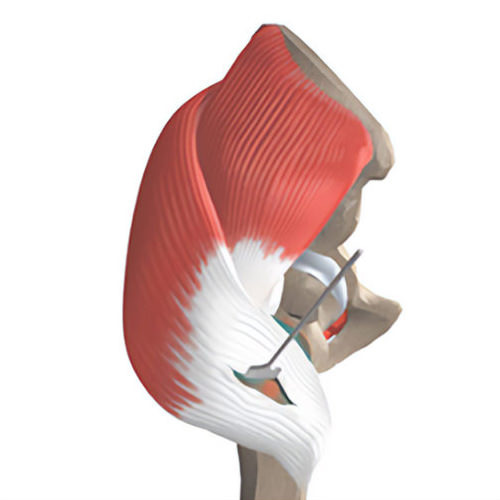
SUPER Hip
SUPER Hip surgery can treat congenital femoral deficiency (CFD). Depending on the classification of CFD, patients may require attention to both the hip and knee joints.
- One long S shaped incision is made that runs from the iliac wing to approximately one-third way down the femur laterally and then back towards the patellar tendon.
- While carefully avoiding nerves, your surgeon will split the fascia longitudinally.
- Soft tissue releases are performed at this time to relieve any contractures.
- Reconstruction of ligaments may be planned with the use of the patient’s own tissues called the fascia lata.
- Next the femoral head and neck is place in a correct orientation by breaking the femur bone and fixing it using plates or rods.
- A pelvic osteotomy (bone cut) is then performed to level the angle of the pelvis and correct any underlying hip dysplasia.
- Further tendon repair and closure is performed.
- The patient is usually placed in a SPICA type cast (to hold the hip and leg in place)
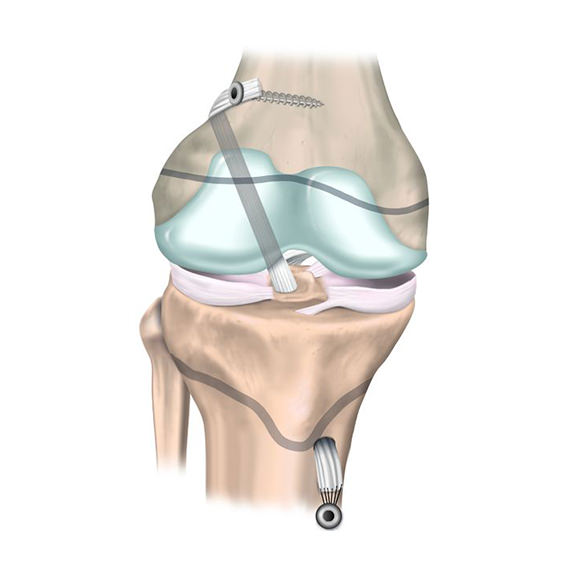
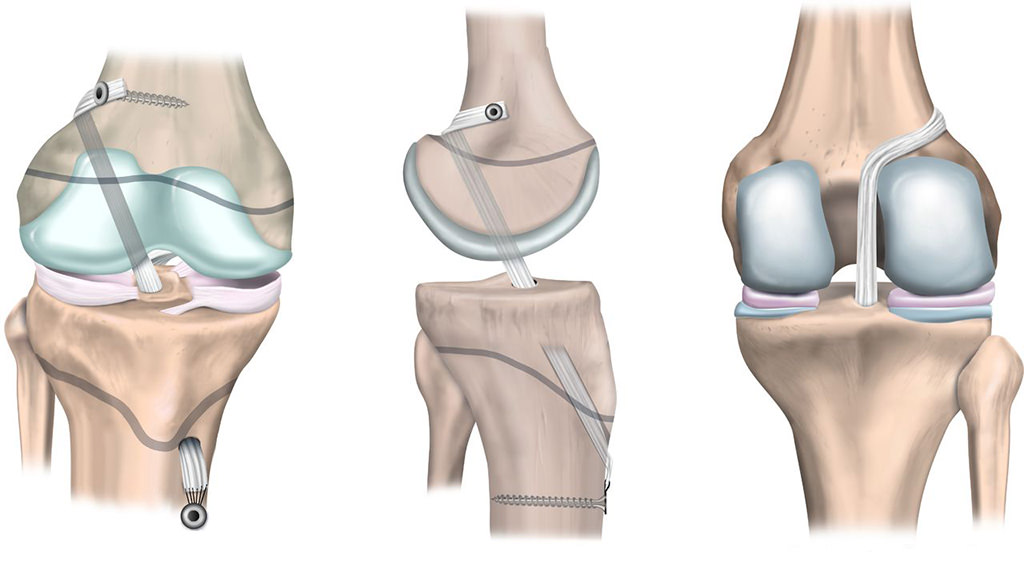
SUPER Knee
- An S shaped incision is made to access the structures of the knee.
- Facia lata is taken and used to reconstruct the ACL and PCL ligaments.
- If patellar (kneecap) mal tracking is present, then the patellar tendon can be realigned.
- Further release of soft tissues in the back of the knee can help correct flexion contractures of the knee.
- After these corrections, the knee will be stabilised and allows for safer limb lengthening procedures to be performed with additional surgeries if necessary.
- The incision is closed.
SUPER Ankle
SUPER Ankle surgery is usually used to treat fibular hemimelia (FH). In some cases, patients will need both reconstruction and lengthening surgeries, that may be performed separately, or in conjunction with one another.
- Different classifications of FH may require different protocols.
- First your surgeon will remove the fibrous fibular anlage. This is a remnant of fibular bone that causes the ankle to be pulled into a valgus deformity.
- Your surgeon will then lengthen the peroneal and Achilles tendons.
- In cases of talo-calcaneal coalition, the talus and calcaneus bones of the foot are separated and reshaped to promote an increased range-of-motion at the subtalar and ankle joints.
- An osteotomy (bone cut) is made at the level of the distal tibia to correct any ankle deformities.
- A bone graft is inserted if needed, into this cut to create a wedge that corrects the angle of the ankle joint.
- The ankle is fixed in place using internal pins.
- When lengthening is also being performed, an external fixator is attached during surgery and an osteotomy is preformed higher up on the tibia.
- Lengthening occurs outside of the operating room, using a gradual adjustment schedule.
Results
Early detection and proper treatment of CFD and FH can lead to very functional and comfortable outcomes for our patients. With reconstructive treatment we can provide patients with functional joints and limbs and allow for future lengthening procedures which would avoid alternative treatments such as amputations. After treatment patients have improved gait and range of motion as well as decreased pain. Our patients see improvements in quality of life and function after surgery.


Potential Complications
As with any surgical procedure, reconstructive surgeries of the hip, knee and ankle can have difficulties and complications. In most cases, our team of specialist can address these concerns without compromising the end results or outcome. Complications and side effects may include:
- Infections
- Wound healing problems
- Malunion or non-union
- Deformities of bones or joints
- Subluxation of joints
- Arthritis
Case studies

AM I A CANDIDATE?
Are you experiencing an orthopedic condition and would like to improve your physical capabilities?
Or you simply would like to achieve your long-lasting dream of improving your height?
Let us help you achieve your optimal health and wellness in a professional setting.
Let’s open up a discussion to help you achieve your goals.
Highly specialized expert care at CLLC
At the Canadian Limb Lengthening Centre we offer complex deformity correction and limb lengthening surgeries performed by experienced surgeons with the most up to date technologies. When it comes to your care, and treatment of deformity and limb length discrepancy, our surgeons have extensive training and experience.
